““I received the SRA/SRT Treatment Chart Books yesterday morning. I am impressed with the high quality of the work and the way they are laid out. I had four SRT sessions yesterday and was able to quickly access all the info I needed and do cross referencing. Thanks again!”
Show your colleagues and associates where and how you want to be treated by using the most advanced nerve, muscle and joint treatment protocols available anywhere! Better still, encourage them to become trained and certified in SRA or SRT!
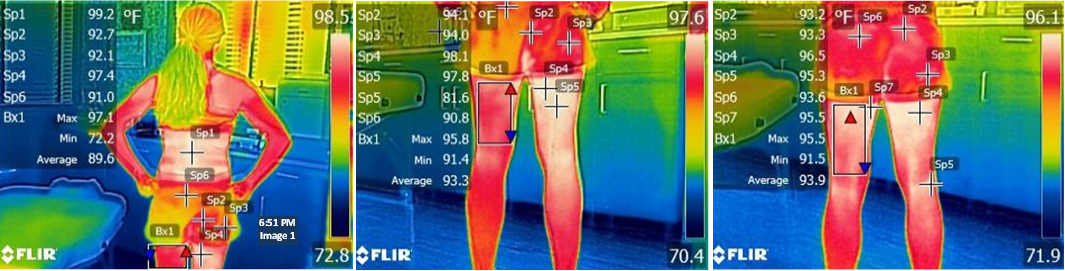
Designed by Dr. Frank Jarrell over 25 years of study and research, Spondylogenic Reflex Syndrome Charts include illustrated images of soft tissue therapy maps, laser therapy points, Chiropractic adjusting and sequencing, Physiotherapy soft tissue and hard tissue manipulation patterns, TrueCore spinal stabilization exercises, dermatome, sclerotome and myofascial pain charts, spondylogenic reflex symptom lists and much more!
For all Health Care Providers interested in the prevalent cause of nerve, muscle and joint dysfunction and pain, these illustrated treatment chart books are great visual aids into exploring this powerful, predictable and reproducible procedural system*.
For certified SRA/SRT providers, a set of printed treatment charts are great for review, furthering your understanding and client education. They also protect you from periodic and frustrating problems with internet access or power outages.
Each volume of the three volume set has a soft cover, full color imaging, 8.5 x 11 sizing, thick and durable paper weight with gloss finish, 175+ pages and large spiral binding for ease of use.
Each volume can be bought individually or as a 3 Volume set and is available to all professions and educators wishing to explore the intimate relationships between the spondylogenic reflex, its pathological sequela and the fundamental zones of treatment.
SRA/SRT Treatment Charts - Volume 1
Biomechanics & Posture
Spinal Reflex Therapy (SRT)
Symptom Lists
SRA/SRT Treatment Charts - Volume 2
Reflex Ladders
Neuromechanics
Laser
SRA/SRT Treatment Charts - Volume 3 includes:
Muscle Testing
TrueCore Stabilization
SRA/SRT Treatment Charts - Volume 4 (coming soon)
Effector Target Tissue Nutrition
Mind-Body Correlates
* These are illustrated SRA/SRT treatment chart books and do not contain or convey assessment, diagnostics and/or treatment procedures. SRA or SRT Training and Certification programs can be purchased separately.